Forehead Contouring
Refines the forehead and brow contour to soften the upper face.
Forehead contouring is a very important part of facial feminization.
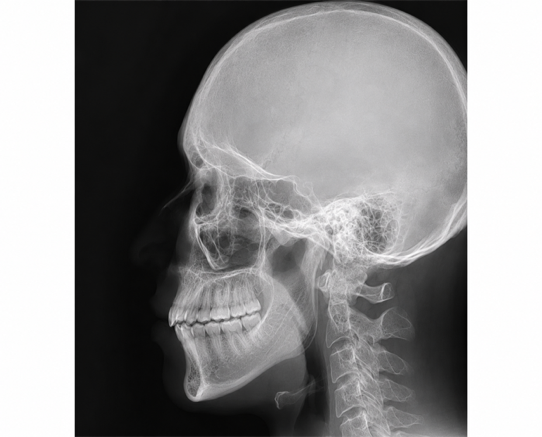
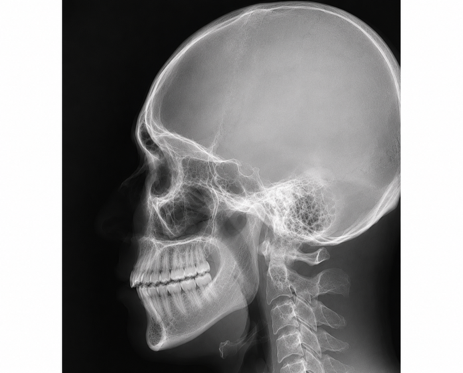
Forehead bony anatomy varies widely in Asian patients. In addition to frontal bossing, the following factors should also be considered:
- Frontal sinus size
- Forehead curvature
- Brow ridge depth
- Nasofrontal angle
- Overall facial proportion
- Personal preference (natural contour / more projected contour)
Therefore, not every patient is suited to the same technique. Forehead contouring is generally categorized into three types.
Type I
Minimal or absent frontal sinus
- Features: thick frontal bone, little or no frontal sinus space, and minimal brow prominence.
- Preferred approach: burring/contouring only, without osteotomy.
- Advantages: shorter operative time, faster recovery, and less swelling.
Type II
Frontal sinus present, but mild prominence
- Features: frontal sinus present, mild brow prominence, and relatively smooth bony contour.
- Preferred approach: burring; depending on needs, Gore-Tex, custom implant, or fat grafting may be added.
- Common goals: improve forehead roundness, correct contour depression, and soften brow lines.

Type III
Prominent frontal sinus and brow bossing (most common)
- Features: most common in Asian transfeminine patients; large frontal sinus with thin anterior wall and clear brow prominence.
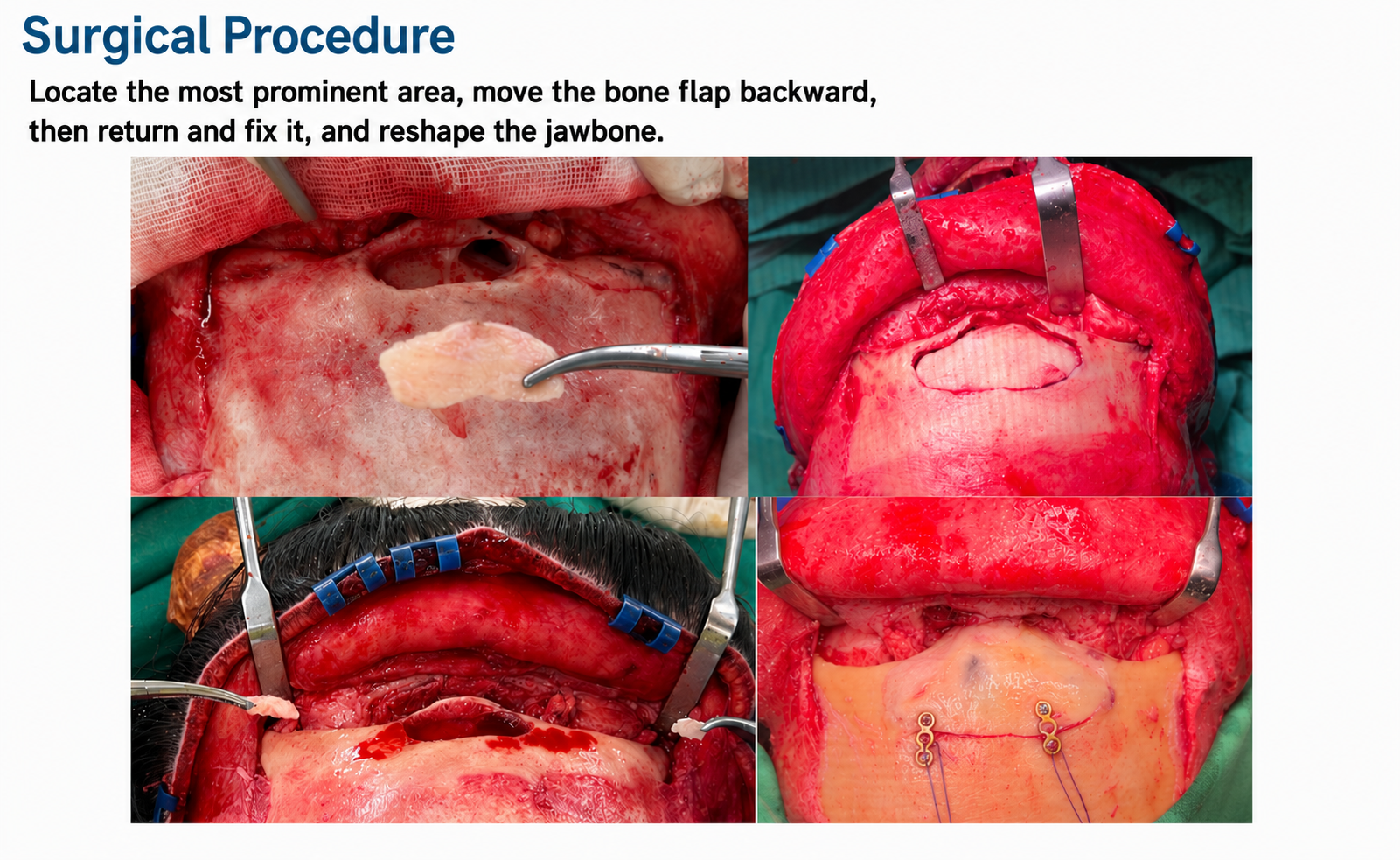
- Preferred approach: osteotomy, anterior wall setback, and fixation with titanium plates.
- May be combined with: forehead fat grafting, bone graft/implant, or hairline advancement.
- Advantages: greatest degree of change, major softening of profile lines, and reduction of masculine brow prominence.
Common combined procedures
- Rhinoplasty: improves nasofrontal transition and overall facial projection.
- Hairline advancement: shortens forehead proportion and enhances feminized framing.
- Brow lift: softens brow-eye distance and upper-face expression.
- Temple/forehead fat grafting: increases smooth roundness and youthful contour.
- Limited hair transplantation: can refine the hairline and improve M-pattern recession.
Important concept in Asian forehead contouring
For many Asian patients, the goal is not simply “flatter is better,” but rather:
- Preserve a natural smooth arc
- Maintain feminine three-dimensionality
- Avoid over-flattening
- Keep harmony with nose, brows, eyes, and hairline
Therefore, technique selection is based on:
- Bone thickness
- Frontal sinus size
- Soft tissue thickness
- Personal aesthetic preference
The final plan is customized for each patient.
Possible complications of forehead contouring
Forehead contouring (frontal bone remodeling) is part of craniofacial reconstructive surgery. Most patients recover well, but the following risks and complications may still occur:
Wound and recovery related
- Swelling and bruising: most common; usually improve over 1–2 weeks.
- Scalp numbness: often due to traction on scalp nerves; typically recovers over weeks to months.
- Scar concerns: may include hypertrophic scarring, visible hairline scar, or temporary alopecia.
Bone and frontal sinus related
- Frontal sinus violation: more common in Type II and Type III; usually repairable intraoperatively, but may increase infection risk in some cases.
- Surface irregularity: may include asymmetry, localized contour unevenness, or palpable edges; revision may be needed in selected cases.
- Palpable fixation material: thin patients may feel titanium plates.
Infection related
- Wound infection: uncommon, but may require antibiotics and wound care.
- Frontal sinusitis: if sinus drainage is suboptimal, chronic sinus discomfort may occur in rare cases.
Nerve and function related
- Temporary frontalis weakness: may occur from dissection and swelling, and usually improves over time.
- Sensory change: some patients may experience tingling, tightness, or altered sensation.
Aesthetic related
- Over-flattened or over-projected forehead: inappropriate planning may produce an unnatural arc or poor nose-forehead proportion.
- Residual asymmetry: natural baseline asymmetry exists, so minor side-to-side differences may remain after surgery.
Type III-specific risk profile
- Because Type III involves osteotomy, setback, and titanium fixation, it usually requires longer operative time, has more noticeable swelling, and involves a longer recovery period, but also offers the greatest degree of correction.