Intestinal Vaginoplasty (Sigmoid Vaginoplasty)
Uses the sigmoid colon to create the vaginal lining, providing stable vaginal depth and natural secretion function. It is currently one of the most common intestinal vaginoplasty techniques.
It is particularly suitable for patients with insufficient original tissue, patients who have undergone failed vaginoplasty and require reconstruction, or patients who wish to obtain more stable vaginal depth.
Main Advantages
- Natural lubrication function
- More stable vaginal depth
- Good tissue thickness, less prone to contracture
- Less likely to rapidly lose depth due to stopping dilation
- Vaginal appearance and texture close to native female vaginal mucosa
- Suitable as a primary or revision vaginoplasty procedure
Suitable Candidates
- Those with insufficient penile and scrotal tissue
- Those who have received puberty blocker treatment
- Those who require reconstruction due to insufficient vaginal depth
- Those who have undergone failed or narrowed penile inversion vaginoplasty
- Those who wish to obtain more stable depth and natural lubrication
Possible Limitations
- Requires abdominal surgery
- Longer operative time
- Longer hospital stay
- In the early postoperative period (3–6 months), there may be more mucus secretion
- Regular follow-up and dilation training are still required
Possible Complications
- Leakage at the intestinal anastomosis
- Intestinal obstruction or intra-abdominal adhesions
- Wound infection
- Vaginal opening stenosis
- Mucosal prolapse
- Excessive mucus secretion
- Rare vaginal perforation or intra-abdominal infection
Operative Time and Recovery Period
- ⏱️ Operative Time: Approximately 6–10 hours
- 🏥 Hospital Stay: Approximately 5–10 days
- 🔄 Recovery Period: Approximately 6–8 weeks
- 📏 Time to Start Dilation: Approximately 10–14 days after surgery
Features of Our Center
- Uses 3D laparoscopy or da Vinci robotic minimally invasive approach to harvest 12–15 cm of sigmoid colon
- Simultaneous vulvar and clitoral reconstruction
- ICG fluorescence blood flow assessment to ensure bowel segment perfusion
- Gender-ERAS™ accelerated recovery protocol
- Provides long-term follow-up of vaginal depth, sensation, and sexual activity
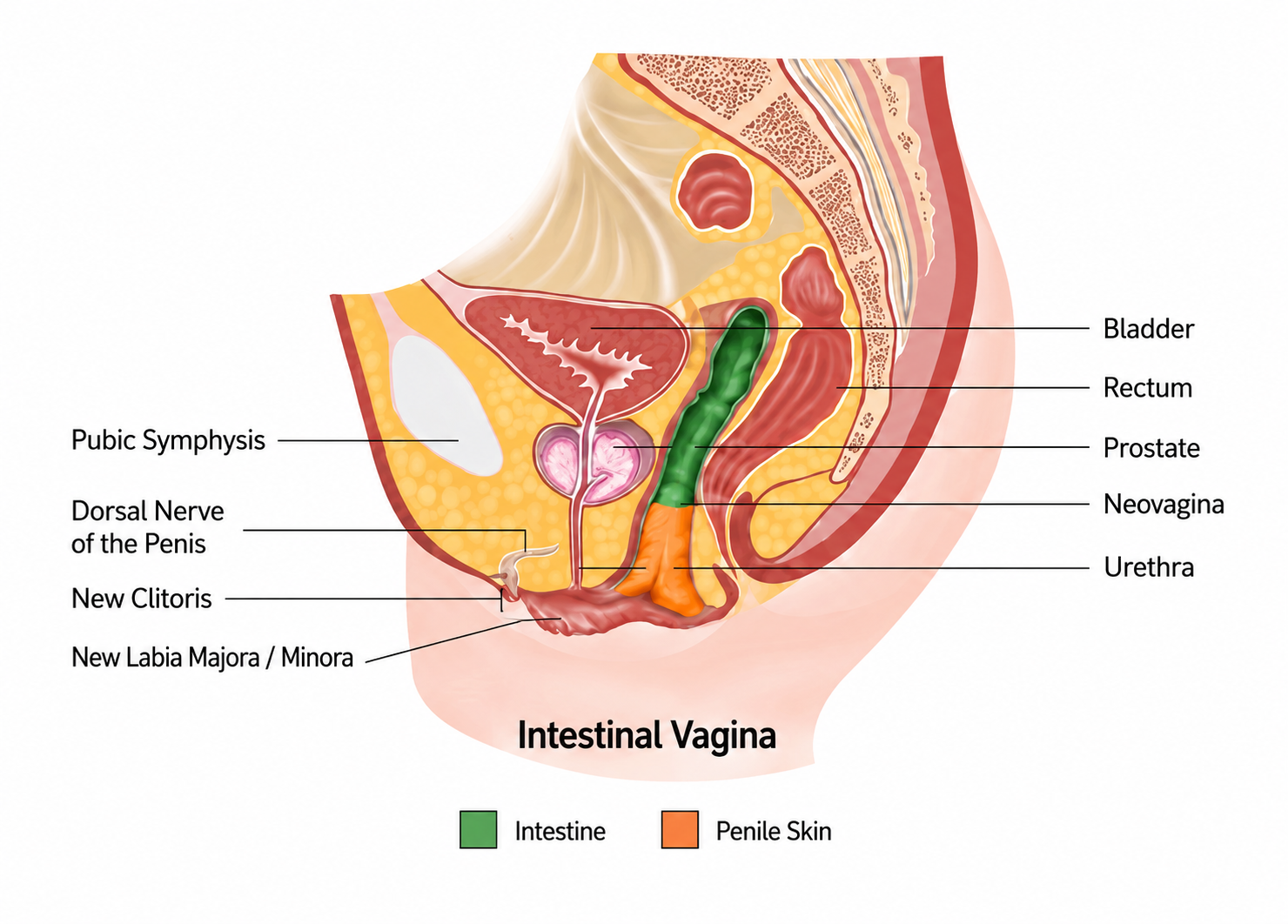
Postoperative Neovagina Schematic
Key points
- Natural lubrication function
- More stable vaginal depth
- Good tissue thickness, less prone to contracture
- Suitable as a primary or revision vaginoplasty procedure