Top Surgery (Top Surgery / Masculinizing Chest Surgery)
For many transgender men, top surgery is not only the removal of breast tissue, but also an important process of establishing a masculinized chest contour.
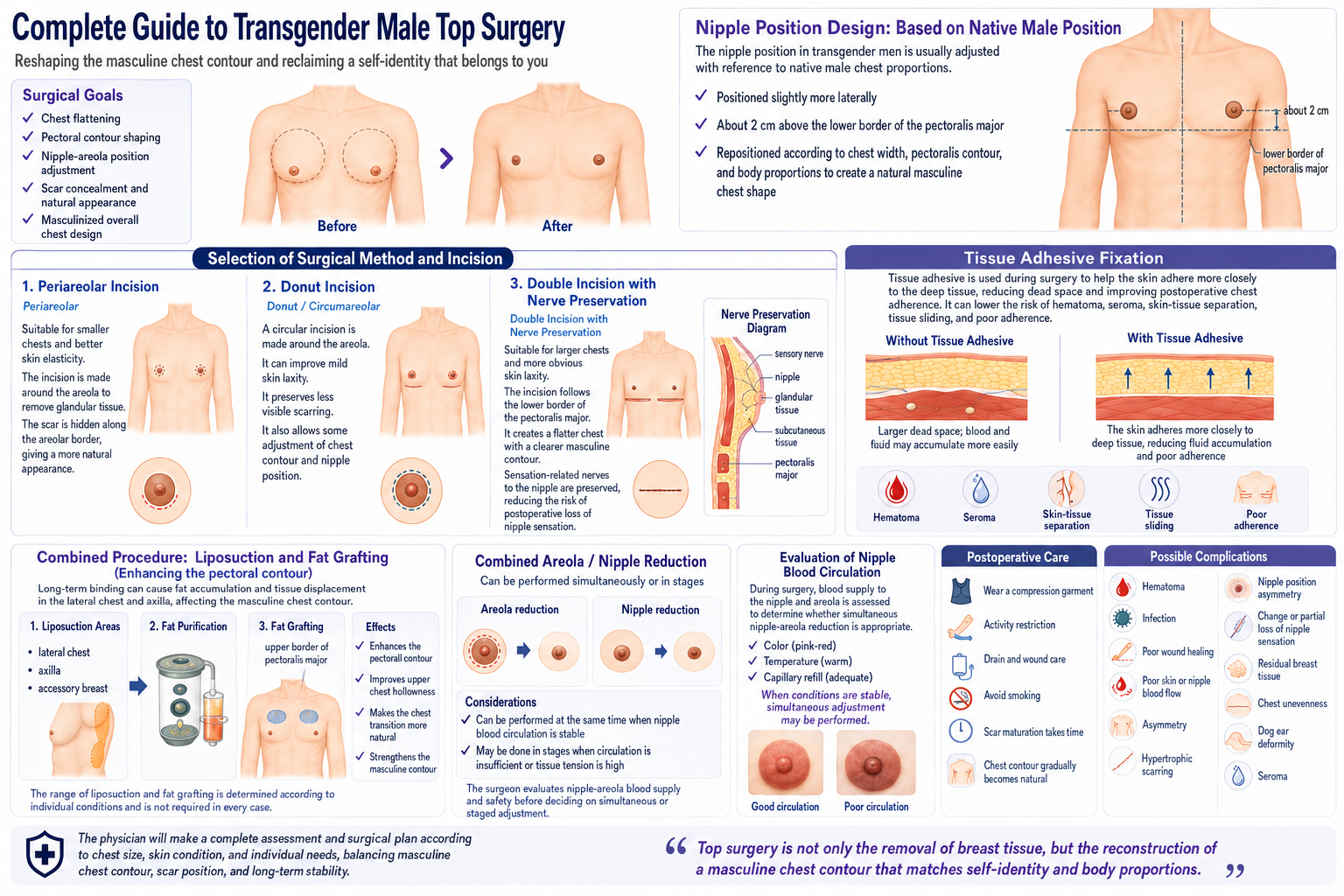
The surgical goals, in addition to flattening the chest, also include shaping the lines of the pectoralis major muscle, adjusting the nipple-areola position, hiding scars, and masculinized design of the overall chest proportion.
Because each individual's chest size, degree of skin laxity, nipple position, and skin elasticity are different, it is necessary to choose an appropriate surgical method and incision design according to personal conditions.
The planning of nipple position for transgender men also needs to be adjusted with reference to the proportions of the cisgender male chest.
Compared with cisgender women, the male nipple position is usually more lateral and is approximately located about 2 cm above the lower edge of the pectoralis major muscle. Therefore, during surgery, the nipple position will be repositioned according to chest width, the contour of the pectoralis major muscle, and body proportion, in order to establish a more natural masculinized chest shape.
"Top surgery is not only removing the breasts, but reconstructing a masculinized chest contour that conforms to self-identity and body proportion."
Surgical Methods and Incision Selection
Periareolar Incision (Periareolar Technique)
Suitable for individuals with a smaller chest and better skin elasticity.
Through an incision around the areola and removal of glandular breast tissue, the scar can be hidden at the areolar border, and the appearance is more natural.
However, for those with a larger chest or obvious skin laxity, it may be more difficult to achieve ideal flatness and a masculinized contour.
Donut Incision (Donut / Circumareolar Technique)
A circular incision is made around the areola, combined with tightening of the surrounding skin, which can improve mild to moderate skin laxity problems.
While retaining fewer scars, it can also perform a certain degree of chest-shape modification and nipple-position adjustment.
Double Incision with Nerve Preservation (Double Incision with Nerve Preservation)
Suitable for individuals with a larger chest, more obvious skin laxity, or who hope for more distinct chest-shape lines.
The incision is designed according to the lower edge of the pectoralis major muscle, which can more naturally simulate the lower-edge line of the male pectoralis major muscle and establish a flat chest shape with a masculinized contour.
During surgery, the sensation-related nerves of the nipple are preserved, with the goal of taking both chest-shape reconstruction and nipple-sensation preservation into account, and reducing the problem of sensory loss that may occur after traditional free nipple grafting.
At present, the traditional double-incision method combined with free nipple grafting is used less often, in order to pursue a more natural appearance, blood-flow stability, and the effect of sensation preservation.
Tissue Adhesive Fixation (Tissue Adhesive Fixation)
During surgery, tissue glue may be used in combination, so that the skin and deep tissue adhere more closely and the formation of postoperative dead space is reduced.
This technique can be applied in different top-surgery methods and helps reduce:
- Hematoma
- Seroma
- Separation of skin and underlying tissue
- Tissue sliding
- Poor chest adherence
At the same time, it can improve the degree of adherence between the skin and chest wall, making the postoperative chest-shape contour flatter and more natural, and helping with stability during the recovery period.
Commonly Combined Surgery: Lateral Chest and Axillary Liposuction (Chest & Axillary Liposuction)
Some transgender men, because of long-term binding, may easily develop fat accumulation at the lateral chest and underarm area, obvious accessory breast tissue, or displacement of skin tissue, making the outer contour of the chest thicker and affecting the masculinized lines after top surgery.
Therefore, top surgery is often combined with lateral chest and axillary liposuction (Lateral Chest & Axillary Liposuction). By adjusting the lateral chest and underarm contours, it improves the outward-spreading appearance and residual fat accumulation, making the transition of the chest shape more natural.
In addition, part of the extracted fat can be purified and then grafted back to the upper-chest area, used to increase the sense of contour at the upper edge of the pectoralis major muscle, making the chest-wall lines closer to the appearance of cisgender male pectoral muscles and improving the overall three-dimensionality and masculinized proportion.
Through the integrated design of glandular breast tissue removal, chest-shape reconstruction, liposuction, and fat sculpting, the postoperative chest is not only "made flat," but rather a more natural and coordinated chest shape with a masculinized muscular contour is established.
Combined Areola / Nipple Reduction Surgery (Nipple-Areolar Reduction)
Some transgender men, because their original areola is larger or the nipple is more protruding, may still retain more feminine chest characteristics after top surgery.
Therefore, top surgery can often be combined with areola and nipple reduction surgery, to readjust the size, proportion, and shape of the nipple-areola, making it more consistent with the appearance of a cisgender male chest.
Areola size, nipple protrusion, and position will be custom-designed according to chest width, the contour of the pectoralis major muscle, and overall body proportion, in order to achieve a more natural masculinized chest shape.
Areola and nipple reduction can be performed at the same time as top surgery, or, according to the nipple blood-circulation condition, skin tension, and postoperative recovery condition, a staged adjustment method may be adopted, in order to take wound healing, nipple survival rate, and overall appearance stability into account.
Postoperative Care
- Postoperatively, a chest compression garment needs to be worn to reduce swelling and assist chest-shape adherence.
- In the early postoperative period, there may be swelling, tightness, and localized numbness.
- Avoid large-range stretching of the upper limbs, weight training, and strenuous exercise for several weeks.
- Perform drain care and wound cleaning according to the physician's instructions.
- Avoid smoking and nicotine use, in order to reduce the risk of poor wound healing.
- Scar maturation usually requires several months to one year to gradually stabilize.
- Chest shape and the degree of skin adherence will gradually become more natural over time.
Possible Complications
Any surgery has certain risks. Possible complications of top surgery include:
- Hematoma
- Infection
- Poor wound healing
- Poor blood flow of the skin or nipple
- Left-right asymmetry
- Scar hypertrophy
- Asymmetry of nipple position
- Change in nipple sensation or partial sensory loss
- Residual breast tissue
- Unevenness of the chest
- Dog ear deformity (bilateral protrusions)
- Seroma
- Poor skin adherence
The physician will conduct a complete evaluation and surgical-method planning according to chest size, skin condition, and personal needs, in order to take masculinized chest shape, scar position, and long-term stability into account.