Breast Augmentation
For transfeminine patients, implant planning is customized to chest framework and soft-tissue conditions to build a natural, proportional breast contour.
For many transfeminine patients, breast shape is not only a body-contour change but also an important part of gender affirmation and self-image.
Because chest anatomy differs from cisgender female anatomy, breast augmentation requires individualized planning rather than simply placing an implant.
Breast augmentation is not only about cup size. It is about finding the right balance among body proportion, soft contour, and gender affirmation.
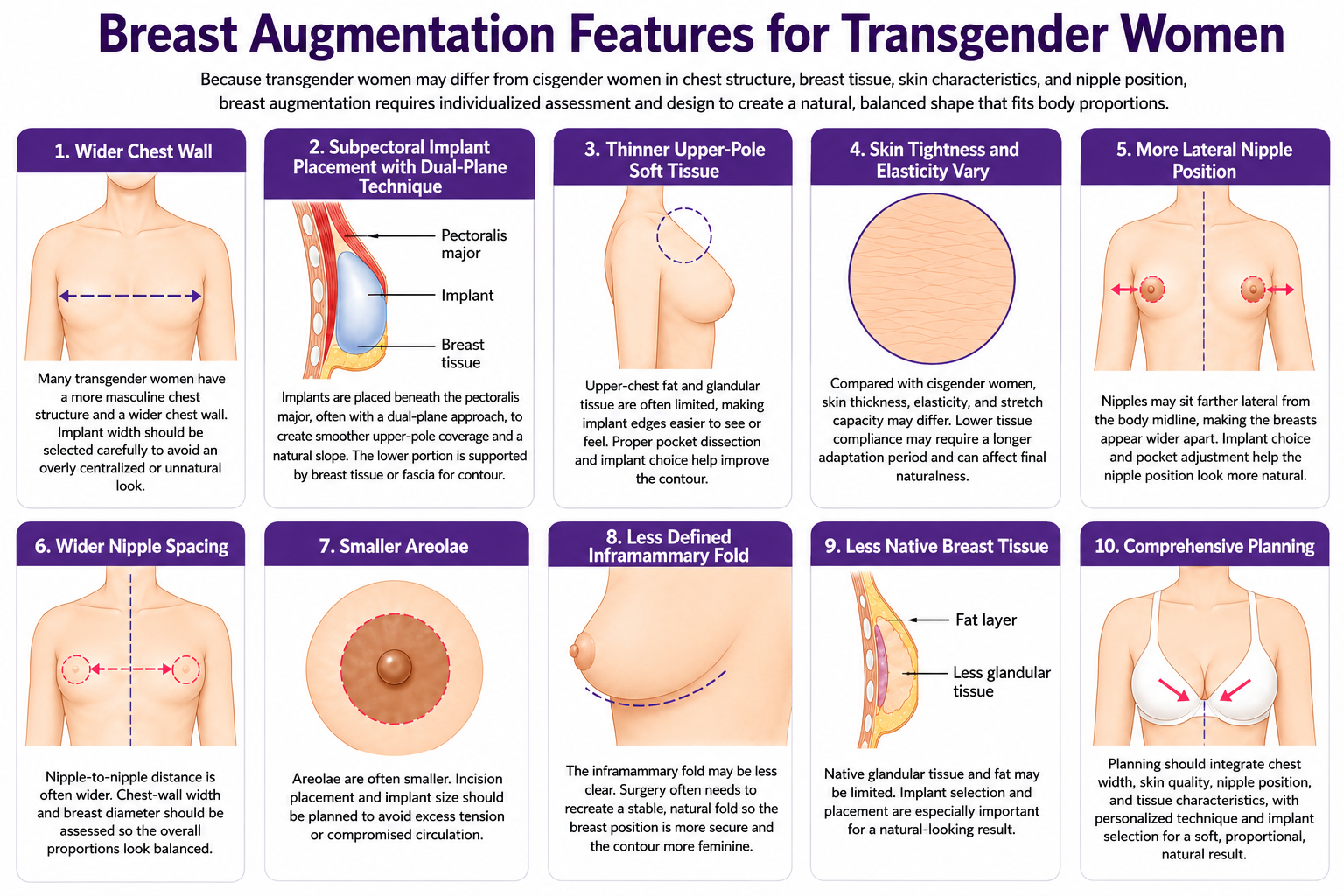
Key anatomic considerations in transfeminine augmentation
Compared with cisgender female patients, transfeminine patients more often present with a wider chest frame, thicker pectoral muscle, thinner upper-pole soft tissue, and wider nipple spacing.
Implant dimensions, projection, pocket plane, and cleavage design should therefore be evaluated with a dedicated transfeminine framework to reduce lateralization, visible edges, and unnatural contour.
- Broader chest framework
- Thicker pectoral muscle
- Thinner upper-pole soft-tissue coverage
- Different skin elasticity and expansion behavior
- More lateral nipple position
- Wider inter-nipple distance
- Smaller areola diameter
- Less defined inframammary fold
- Limited native breast tissue
Incision options
Incision planning depends on areola size, chest anatomy, implant size, and scar preference.
- Transaxillary approach: incision is hidden in the axillary crease and avoids a breast scar; useful for smaller areola, but requires higher technical precision for symmetry and position control.
- Inframammary fold approach: provides broader exposure and more precise dissection, and allows fold definition or adjustment; often stable for broader chest frames or larger implants.
- Periareolar approach: scar may blend with the areolar border, but a small areola can limit delivery of larger implants.
Implant surface and pocket plane
Silicone implants are most commonly used and are selected based on softness, support requirement, chest dimensions, and tissue thickness.
- Smooth implant: softer feel and more natural mobility, but some patients may have higher risk of displacement or bottoming out.
- Microtextured implant: fine surface texture can improve positional stability and reduce rotation or displacement risk in selected patients.
- Submuscular placement: improves upper-pole coverage and can reduce visible edge or rippling, especially when native tissue is limited.
- Dual-plane technique: combines submuscular and glandular-plane adjustment to balance natural slope and lower-pole fullness.
Pure subglandular or subfascial placement is often less suitable in many transfeminine cases because visible edge, rippling, or contour instability may be more likely.
Intraoperative illustration
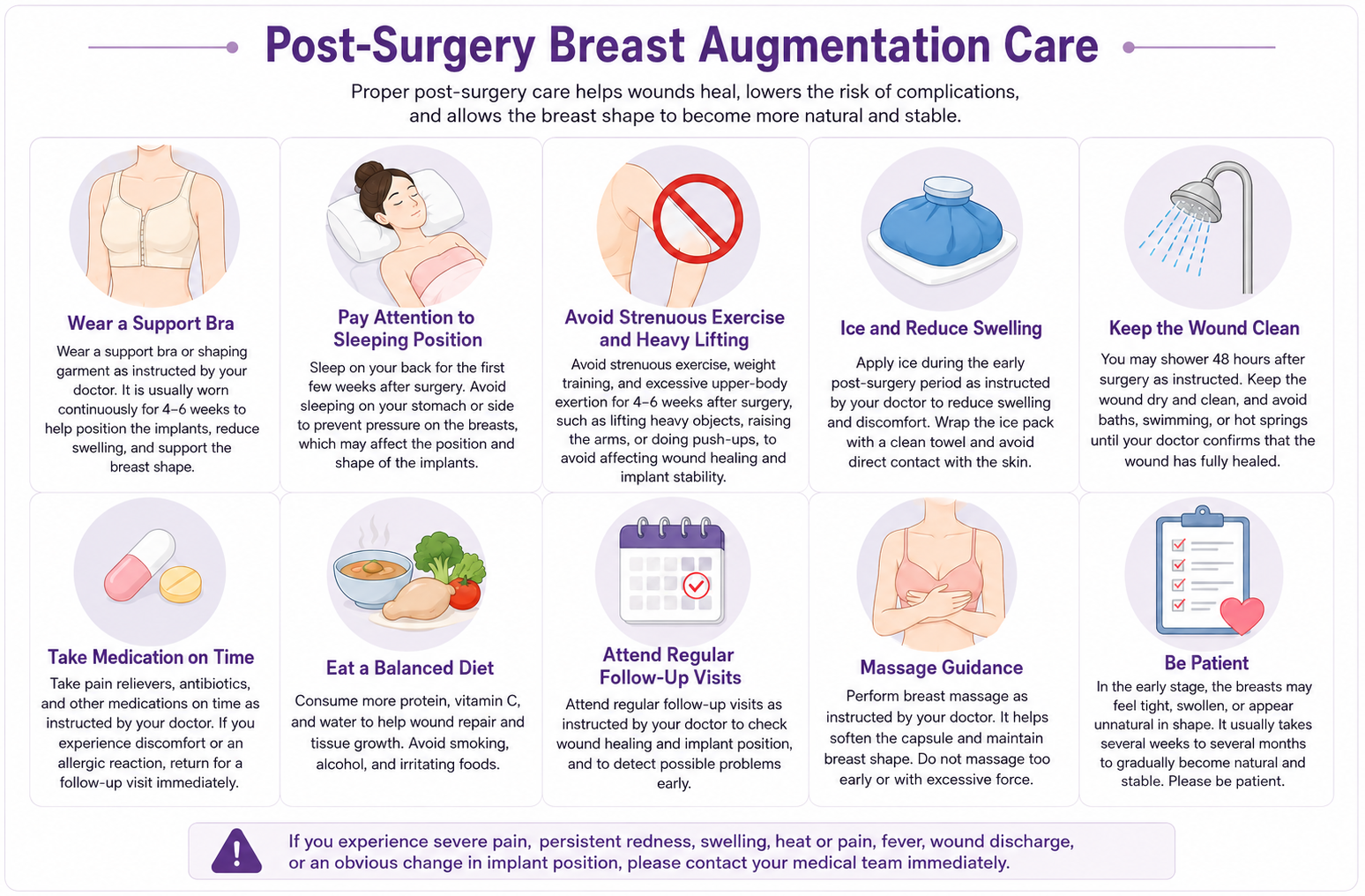
Postoperative care
- Early swelling, tightness, pressure sensation, and mild pain are common and usually improve over time.
- Wear postoperative support garments as instructed to help implant stabilization and contour shaping.
- Avoid strenuous exercise, heavy upper-body training, and forceful arm activity during early recovery.
- Avoid prone sleeping and direct chest compression.
- Attend scheduled follow-up visits to monitor wound healing, implant position, and contour progression.
- Final softness and contour usually evolve over several months up to around half a year.
- Massage and aftercare protocols should be tailored to implant type and surgeon guidance.
Potential complications
All surgery carries risk. Individual assessment of tissue thickness, chest proportion, and soft-tissue support helps reduce complications and improve long-term stability.
- Hematoma
- Infection
- Capsular contracture
- Implant displacement
- Bottoming out
- Asymmetry
- Rippling
- Delayed wound healing
- Sensation change
- Implant rupture or leakage
- Lateral breast drift or limited cleavage
Key points
- When the chest is broader, pectoral muscle is thicker, and soft-tissue coverage is thinner, implant width and pocket depth must be recalculated.
- When nipple position is more lateral and inter-nipple distance is wider, cleavage design and breast centerline need dedicated planning.
- Incision, implant surface, and placement plane should be selected together to balance natural appearance and long-term stability.